


Introduction
After appearance of the novel Coronavirus 2019 in Wuhan, China, new epicenters of the now pandemic appeared nationally. The new Coronavirus disease 2019 (COVID-19) is associated with a syndrome of acute hypoxemic respiratory failure that can lead to admission to intensive care unit (ICU), invasive mechanical ventilation, and at times, death. The first two COVID-19 cases in the State of Michigan were reported in March 10, 2020. During the subsequent weeks, Michigan became one of the early national epicenters of the current COVID-19 pandemic. Early observational studies have suggested a correlation between susceptibility to COVID-19 infection and type A blood group, and furthermore, increased risk of respiratory failure and worse outcome. We conducted this retrospective study to evaluate the association between ABO blood groups and disease severity/mortality in hospitalized COVID-19 patients.
Methods
We reviewed the records of hospitalized patients with PCR-confirmed COVID-19 testing managed at Henry Ford Health System (HFHS) between March 10 and April 30, 2020. Henry Ford Health System (HFHS) serves inner city and metropolitan Detroit in Michigan, with diverse demographics including African American, Middle Eastern, and Caucasian populations. Age, gender, race, ABO blood groups, comorbidities, disease severity (defined as intensive care unit admission), intubation, and mortality variables were collected for 1488 eligible patients. Survival data was updated on July 15, 2020.
Results were presented as median plus range, or percentages as indicated. In the univariate analysis, Student's t-test and Pearson's Chi-square/Fisher's exact test were used to determine the significance and odds ratio (OR) for the independent variables as related to outcome. A multivariate analysis was performed using logistic regression to identify the risk factors for mortality. A backward stepwise (Wald) selection model was performed, with significance level for removal from the model set at 0.1. All tests of significance were two-sided, and a p value of < 0.05 was regarded as significant. All statistical analyses were performed using SPSS (Statistical Package for Social Sciences) software, version 22 (SPSS Inc., Chicago, IL, USA). This study was approved by the Institutional Review Board of HFHS.
Results
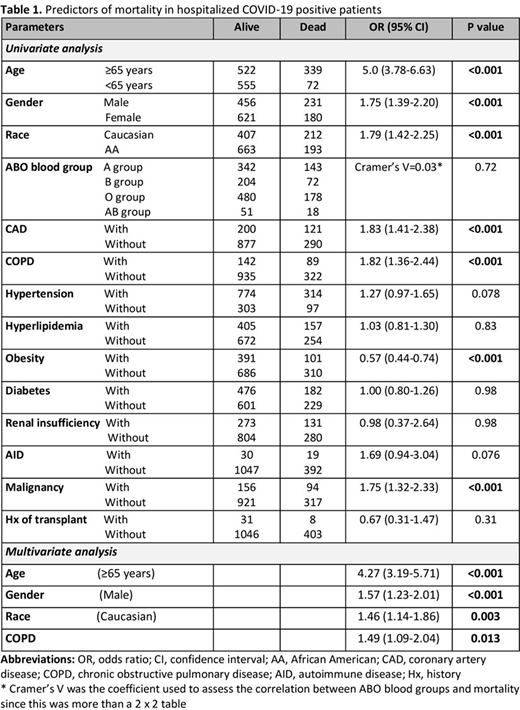
1488 hospitalized COVID-19 positive patients with available ABO blood group were included. The median age of patients was 68 years (Range 19-99 years); 801 (54%) were females. Most patients (n=856; 58%) were African Americans. 485 (32.6%) patients had blood group A, 276 (18.5%) had group B, 658 (44.2%) had group O, and 69 (4.6%) had group AB. 469 (31.5%) patients required ICU admission, 370 of whom were intubated. On last follow up, 411 (27.6%) patients were dead. ABO blood groups and Rhesus factor (D antigen) were not associated with the ICU admission, intubation, or mortality. Male gender, age ≥65 years, some underlying diseases such as obesity, coronary artery disease chronic obstructive pulmonary disease and malignancy were associated with increased mortality. African American patients were almost 40% less likely to die (OR = 0.56; 95% CI: 0.44-0.7; p < 0.001). Table 1 shows the parameters analyzed as predictors of mortality using univariate and multivariate logistic regression. Multivariate analysis showed that age (≥65 years) (OR = 4.27; 95% CI: 3.19-5.71; p < 0.001), male gender (OR = 1.57; 95% CI: 1.23-2.01; p < 0.001), Caucasian race (OR=1.46; 95% CI: 1.14-1.86; p = 0.003), and COPD (OR = 1.49; 95% CI: 1.09-2.04; p = 0.013) were associated with mortality.
Conclusion
According to our study, ABO blood groups and Rhesus factor did not correlate with disease severity, use of mechanical ventilation, or mortality in hospitalized COVID-19 patients. Elderly patients, male gender, patients with COPD were at increased risk of death. Contrary to perceived belief, African Americans were not at increased risk of mortality, compared to Caucasians with COVID-19 infection. Caucasians were more likely to die from COVID-19 infection.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal